Fun day in the OR
I "saved" this post from last Thurdsday, my last day of OB, and I was going to elaborate on the interesting stuff I saw and participated in on my last day...but unfortunately I'm stacked on time, so instead you get some pics below...and explanations of the cases/surgeries to come later.
 Monochorionic (one placenta) diamniotic (two amniotic sacs) twins with twin-to-twin transfer syndrome delivered by C-section:
Monochorionic (one placenta) diamniotic (two amniotic sacs) twins with twin-to-twin transfer syndrome delivered by C-section:
basically the one baby is hogging all the blood and nutrients from the other, so to ensure that both their survival they were delivered earlier
 Cervical spine; not apparent from this picture representation, but our patient had two herniated intervertebral discs (the light blue between the vertebrae above) C5-6 and C6-7 levels leading to compression of some of his nerves
Cervical spine; not apparent from this picture representation, but our patient had two herniated intervertebral discs (the light blue between the vertebrae above) C5-6 and C6-7 levels leading to compression of some of his nerves
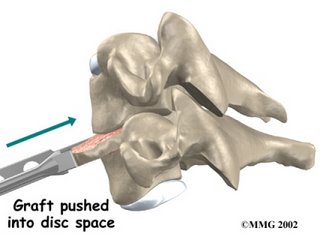 To relieve the pressure on the nerves from intervertebral disc compression, the intervertebral disc is removed the space is filled in with an allograft (bone from a cadavar; usually bone from the hip bone)
To relieve the pressure on the nerves from intervertebral disc compression, the intervertebral disc is removed the space is filled in with an allograft (bone from a cadavar; usually bone from the hip bone)
 Finally it is stabilized with a metal plate anteriorly
Finally it is stabilized with a metal plate anteriorly
 Here is what it can look like on MRI; the arrow is pointed at the herniated disc. The "gray" between the two "white" lines is the spinal cord; the "white" lines on each side represents the spinal fluid and should be continuous, but you can see above that the disc bulges into the fluid and impinges on the cord
Here is what it can look like on MRI; the arrow is pointed at the herniated disc. The "gray" between the two "white" lines is the spinal cord; the "white" lines on each side represents the spinal fluid and should be continuous, but you can see above that the disc bulges into the fluid and impinges on the cord
 Pictorial example of what a herniated disc can look like
Pictorial example of what a herniated disc can look like

 Monochorionic (one placenta) diamniotic (two amniotic sacs) twins with twin-to-twin transfer syndrome delivered by C-section:
Monochorionic (one placenta) diamniotic (two amniotic sacs) twins with twin-to-twin transfer syndrome delivered by C-section:basically the one baby is hogging all the blood and nutrients from the other, so to ensure that both their survival they were delivered earlier
 Cervical spine; not apparent from this picture representation, but our patient had two herniated intervertebral discs (the light blue between the vertebrae above) C5-6 and C6-7 levels leading to compression of some of his nerves
Cervical spine; not apparent from this picture representation, but our patient had two herniated intervertebral discs (the light blue between the vertebrae above) C5-6 and C6-7 levels leading to compression of some of his nerves To relieve the pressure on the nerves from intervertebral disc compression, the intervertebral disc is removed the space is filled in with an allograft (bone from a cadavar; usually bone from the hip bone)
To relieve the pressure on the nerves from intervertebral disc compression, the intervertebral disc is removed the space is filled in with an allograft (bone from a cadavar; usually bone from the hip bone) Finally it is stabilized with a metal plate anteriorly
Finally it is stabilized with a metal plate anteriorly Here is what it can look like on MRI; the arrow is pointed at the herniated disc. The "gray" between the two "white" lines is the spinal cord; the "white" lines on each side represents the spinal fluid and should be continuous, but you can see above that the disc bulges into the fluid and impinges on the cord
Here is what it can look like on MRI; the arrow is pointed at the herniated disc. The "gray" between the two "white" lines is the spinal cord; the "white" lines on each side represents the spinal fluid and should be continuous, but you can see above that the disc bulges into the fluid and impinges on the cord Pictorial example of what a herniated disc can look like
Pictorial example of what a herniated disc can look like
The last case I scrubbed on was a laminectomy of two lumbar levels. In this case, the neuropathy (nerve problem) was due to a narrowing spinal canal (where the spinal cord runs). To relieve the pressure off the spinal cord, a decompression is done through a laminectomy; basically, a window is cut from the back of the vertebrae to air out the cord and give it room
That's all I have for now. I started my orthopedic surgery rotation on Friday, and I've been pretty busy since. The hours suck....not used to getting up at 4:00, but luckily my roomate has to get up the same time, and he doesn't get home until 8:00 or 9:00 at night. The remainder of my immediate schedule consists of being on call this weekend, flying to Philadelphia for a test next Wed through Sunday, and starting up my 2nd from last MBA class.
posted by Jimmy at
6:25 PM
|
2 comments
![]()


